
Articles
April 29, 2025
Cell & Gene Scale-Up: How Supply Chain Design Evolves as a Company Matures
In 2024, AIM published an article exploring the supply chain implications of transitioning from the clinical to the commercial stage in the cell and gene (C&G) therapy space. As one might imagine, advancing to commercial production and distribution brings a lot more complexity. As the number of patients increases, demand becomes less controlled and less predictable. Logistical challenges increase as the number of treatment centers expands. Patient engagement and consent processes, labeling requirements, and order-to-cash processes all become more complex. Meanwhile, physicians and patients will understandably seek the most reliable delivery and best turnaround times, even as complexity rises.
Dealing with that initial transition is challenging. But what about after that? Are all the puzzle pieces set at that transition point, only to remain in place indefinitely? In short, no. Instead, it’s more accurate to view the transition as an ongoing process that persists as the company matures and scales up its operations over time, continually refining and optimizing its supply chain design and set-up. But what should that process look like, and what are some key points to keep in mind?
More recently, our team attended a large conference where several major pharmaceutical companies shared their views on setting up supply chains for cell and gene products. The consensus emphasized leveraging existing capabilities, building new ones where necessary, and starting with automation to avoid reliance on manual processes. These are fair points when backed by a large, established organization. But what happens if a company is entering the cell and gene space without such support?
In this paper we explore the questions above, as well as the implications for cell and gene therapy companies as they evolve through different phases of maturity. We start by outlining considerations for supply chain design and set-up during the initial launch phase. Then, as companies grow, different approaches are required, particularly as they scale up. In this context, we examine how things can evolve across six key capabilities:
- Supply Chain Design and Partner Selections
- GxP Licenses
- Order-to-Cash
- Cell Collection and End Product Delivery
- Risk Management
- Chain of Custody / Identity
Table 1: Supply Chain Evolution Across Six Key Capabilities
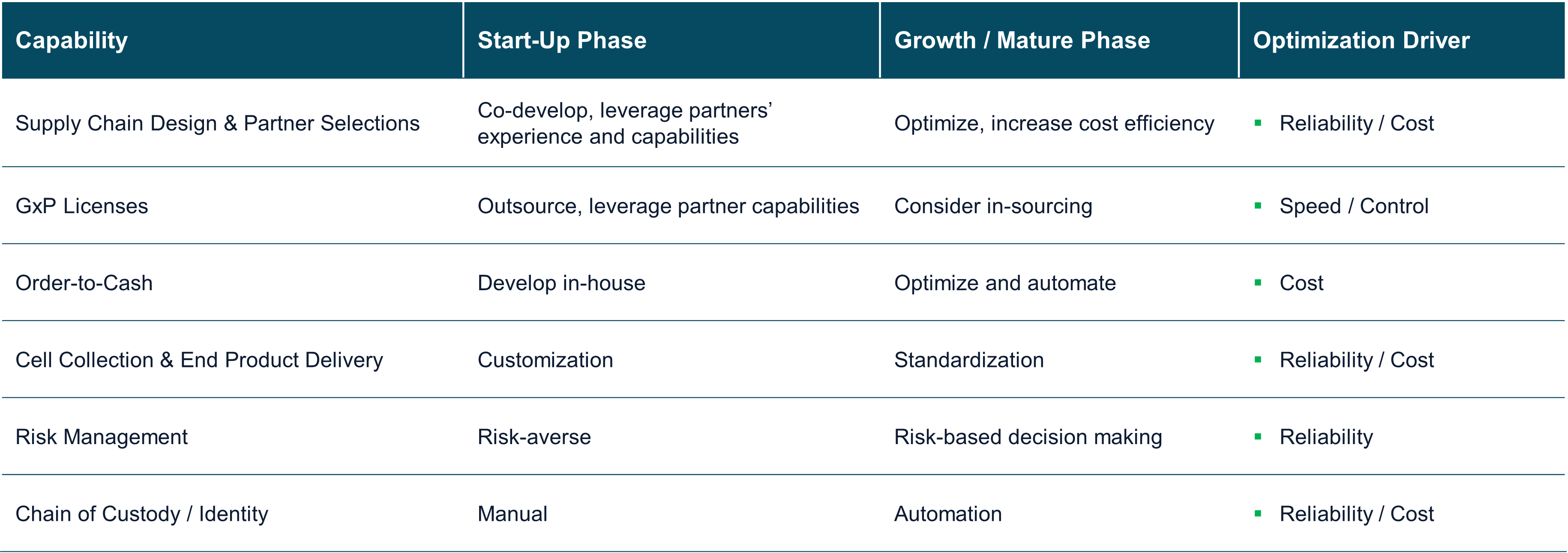
As companies mature, order volumes typically increase. Automation and standardization can offer solutions to manage the growing complexity. However, it is equally important to assess whether the supply chain setup still meets operational needs – and whether changes are needed to ensure timely, reliable delivery and optimal vein-to-vein time. Throughout its growth journey, any company will need to appropriately balance cost considerations with the need for reliability and speed.
The maturity phases mentioned in Table 1 above are loosely defined as Start-Up and Growth / Maturity. Each company’s journey is different, so it isn’t value-added to be more granular at this point. We also focus only on a small number of processes, actions, and external factors. Our intention is to offer context for situations in which it may be valuable to revisit earlier decisions.
Supply Chain Design and Partner Selections
Many C&G companies retain components of their clinical-stage supply chain setup as they transition to commercial operations. While new markets, destinations and customers are added, the overall design is often not reconsidered, as we mentioned in our previous article. The company’s focus is understandably on getting the product on the market to serve patients, and rightfully so. However, it’s important to ensure that the supply chain partners that served the company well in the clinical stage are equally suited to the commercial supply chain.
As companies grow, and as the numbers of patients, customers, and transactions rise, they typically require additional capacity and flexibility. The flip-side is that they typically also become more cost-conscious. Our team has seen clients work effectively with renowned partners in the clinical stage, only to encounter capacity constraints or cost challenges during commercial rollout.
We recommend periodic evaluation of both the business and market supply chain needs. These may indicate that existing partners can continue supporting the company well in the commercial stage with minor adjustments, or they may highlight some serious gaps. In the latter case, and depending on the type of supplier, we recommend assuming approximately six months for selection, qualification, and contracting of a new supplier. In the selection process, it’s key to select a supplier that is flexible and equally invested in delivering on the patient needs and supporting the company’s growth.
GxP Licenses
Pharmaceutical companies entering the European market are often critical of the size of their operational footprint. GxP licensing is a key component of this discussion. At a basic level, a company requires a Manufacturing Importation Authorization (MIA) with a corresponding Qualified Person (QP) market release, as well as a Wholesale Dealer Authorization (WDA) with a corresponding Responsible Person (RP) release.[1]
Many companies—particularly in the start-up phase but also later—opt for leveraging a third party’s MIA. This allows the quality management system to focus on Good Distribution Practice (GDP) to support the WDA, which typically requires less effort to create, maintain and implement.
In the autologous cell therapy space, however, this setup requires careful consideration. From the outset, it is important to understand the QP’s level of autonomy and the flexibility required from a business perspective. We have observed cases where QP availability was limited to regular working hours, resulting in delays that directly affected vein-to-vein timelines. Given the time-sensitive nature of C&G therapies, aligning on working hours and service expectations is critical when working with a partner for MIA and QP services. Our team has seen examples where product release was postponed by several days due to weekend scheduling. While this may be standard practice in traditional pharma, in autologous C&G therapies where every day counts, it can demand a more strategic approach, as delivery, reliability, and turnaround time are crucial.
As volumes increase, the scheduling and execution of EU market release steps—especially if the QP requires physical access to the product—can become a bottleneck. Of course, this is QP dependent and subject to local interpretation of requirements for performing EU market release. From the beginning, we recommend clearly defining all requirements and availability expectations when outsourcing QP services. These requirements are sometimes overlooked during preparation for filing. We suggest regularly reviewing the licensing setup to ensure it still meets the company’s future requirements.
Depending on the state and scope of the quality management system, obtaining an MIA can take 6-9 months. Once granted, the MIA must be added to the EMA dossier to allow the company to “insource” the QP market release activities. Most vendor companies that offer the services described above are also capable of helping develop a quality management system and supporting a license application. In a more mature state, such partners can also serve as a back-up QP for extra capacity or to cover absence of the in-house QP.
Order-to-Cash
For companies setting up operations in Europe, establishing an efficient order-to-cash (O2C) process—either directly or via a partner—can be one of the more complex tasks. EU, and local regulations on ordering and invoicing, market behavior, platform requirements, and language barriers all play a role.
In the C&G space, some of these challenges may be less severe due to the type of customers and the volume of shipments. We can assume (for example) that the centers of excellence that administer these therapies generally operate in English, allowing for simpler communication without the need for using multiple languages. However, regulatory and invoicing challenges still apply.
Transaction volume can also be a double-edged sword. During the early stages of commercialization, companies may process fewer than 50 transactions per year. Order-to-cash partners typically price services on an activity basis, making low volume clients less attractive or more costly per transaction. This could be a challenge for C&G companies that are seeking to outsource this process at an acceptable cost level.
For this reason, setting up an internally managed process may be the best option in the early stages. With limited volume, a company can often handle transactions manually with existing tools. An order often translates directly into a reserved manufacturing slot, determined by either fresh or frozen cell collection. Companies may also need to consider how and when slot availability is shared with treatment centers at the moment of order placement. Having a system in place to share such information–via a portal, for example–is ideal. However, be sure to involve your customers in the design process to avoid potential negative feedback and/or the possible need to rework the solution later.
As commercialization progresses and volumes grow, complexity increases. Local regulations, ordering practices, invoice requirements, and payment behaviors differ by country and will become more complex. Supporting this internally will require more resources (additional FTEs) and the potential need to invest in more advanced technology.
The make or buy decision around the O2C process should be revisited regularly. Technology will play a key role in keeping the process manageable. Implementing automation in order entry, creating a customer portal, and selecting a broker to manage and monitor e-invoicing requirements are just a few things to consider.
However, since order-to-cash processes involve direct interaction with end customers and directly impact vein-to-vein time, it is critical that the process remains reliable through each of the company’s maturity phases.
Cell Collection and End Product Delivery
In autologous therapies, a company must design a process to collect the apheresis material from treatment centers. It is essential that this process ensures cell quality while also being efficient for the treatment center. As companies transition from clinical to commercial supply, the cell collection process is often based on the original clinical design. While suitable for studies, that’s not necessarily scalable.
Many companies start with a passive, patient-specific shipping solution with pre-applied labels. This avoids the need for hospitals to generate their own labels, ensuring that the chain of identity (COI) is preserved. However, as volumes increase, the need to store pre-labelled boxes becomes a logistical challenge. These boxes are supplied well before the apheresis process is performed to allow immediate shipping of the material but take up significant space at the hospital. To address this, companies may allow hospitals to generate labels themselves. This enables a more flexible label, pack, and ship process led by the hospital. The manufacturer must now be equipped to handle inbound shipments prepared by the hospital, requiring alignment on label formats, arrival windows, and COI / chain of custody (COC) standards. It is also key for the manufacturer to ensure all parties apply the same amount of rigor in the COI / COC process to ensure the correct cells arrive against the correct conditions.
Finished cell delivery will likely undergo a similar journey. In the startup phase, as the number of orders is low, a company will probably leverage the experience gained during clinical operations. Often, the company will closely monitor and manage each step of the order journey to ensure that all goes as planned. Delivery is typically white-glove, highly coordinated, and supported by hands-on training for hospital staff. In some cases, the delivery driver may even play a key role in the process. We’ve seen examples where the driver could also train or re-train the staff upon arrival, perform dry runs with the hospital staff to increase the chances of success, and immediately provide the manufacturer with information on the delivery process and any potential events.
While effective, these services are costly. As volumes start to grow, cost-consciousness typically increases. Companies look to work with supply chain partners to scale back services while still striving to maintain quality and reliability. Scaling back might involve non-dedicated transport (e.g. milk runs) or optimized packaging for easier hospital handling. Advanced tracking and real-time temperature monitoring can also help maintain standards while reducing cost.
To ensure the best vein-to-vein time, as well as reliability in pick-up and delivery timing, companies should assess the capabilities of their supply chain partner(s) and ensure they are meeting the requirements of their respective maturity stage.
Risk Management
In C&G, where treatments are time-critical, a structured risk management process is essential. Early on, every order is closely monitored to better understand and quantify risks. As companies grow, they can shift to more proactive risk mitigation strategies. For example, introducing back-up shipping lanes, moving from dedicated vehicles to non-dedicated, switching modes (road to air or vice versa, etc.), or adjusting service levels based on risk tolerance. An example here would be allowing more shipping days or combining shipments in a milk run.
Volume and experience provide valuable data for reassessing the logistics strategy. As a company matures, it gains a much better understanding of the relevant distribution lanes, as well as critical control points. This enables the company to adopt a more informed risk-based approach that can help reduce costs while maintaining quality levels.
For example, some companies reduce service levels while maintaining reliability by moving from white-glove service to parcel delivery on specific routes. With scale, companies should establish playbooks detailing internal and external processes and agreements. These ensure that even when more risk is introduced, performance levels remain high and predictable.
While introducing more risk into your supply chain sounds contradictory, as volumes grow and complexity increases, a risk management strategy that is too risk averse will be challenging to scale up. Companies that understand their supply chain risk, perform regular risk assessments, and actively manage it will be more effective during scale up. Avoiding risk at all costs will be very expensive to sustain and may prevent a company from being flexible and agile enough to adjust to customer expectations.
Chain of Custody / Chain of Identity
COC and COI are critical pillars of any cell therapy supply chain. Multiple solution providers offer reliable tools to manage this. However, they regularly need to be adjusted to fit the company’s specific process. Special care is needed, though. If such development is done in isolation, then it may impact usability for the end customer, particularly for hospitals managing products from multiple manufacturers.
Each manufacturer may offer a different platform, login procedure, or workflow. In one instance, a client selected a leading software system and tailored the platform to anticipated user needs. However, once launched, the company received feedback from the market on the solution they had implemented. Updates were made to the process, but this obviously took time. Additionally, discussions rose within the organization on how well the portal would perform in other parts of the world. Were there more local requirements that should be included? What about language, what would customers prefer?
In a start-up phase, a company might still decide to “handhold” each order and manage the customer experience very closely. As volumes rise, this becomes very labor-intensive with an increased risk of mistakes. Technology becomes essential, but it must be developed with a deep understanding of the market, and ideally, in collaboration with key users. If the solution doesn’t meet user requirements, then it could negatively impact vein-to-vein time and overall customer satisfaction. To help ensure long-term success, a manufacturer needs to proactively consider the user experience early on, then design a robust and user-friendly system that can scale up effectively.
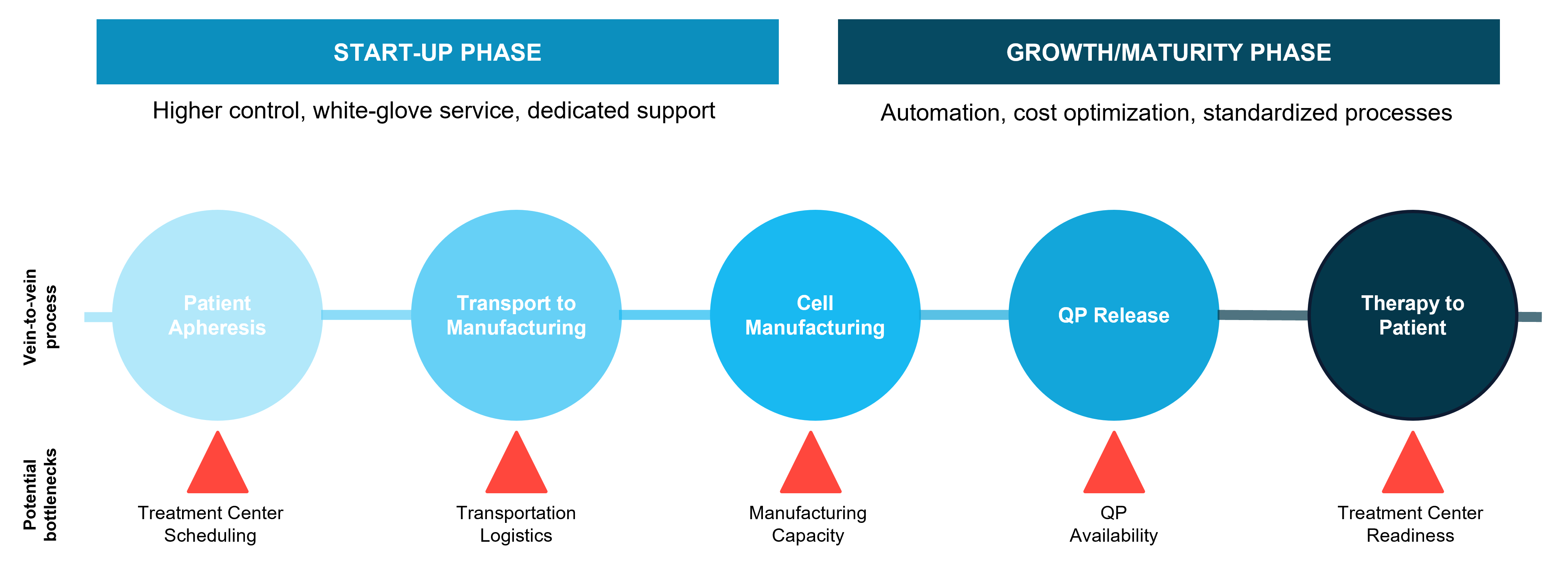
Figure 1: Vein-to-vein process for Cell & Gene Therapy, with potential bottlenecks and timeline impacts
Parting Thoughts
Clearly, making the transition from a clinical supply chain to a commercial supply chain involves a transition process. But the transition doesn’t end there. Rather, it continues through various phases of the company’s evolution.
Physicians and patients will always seek an effective therapy that provides the most reliable delivery and the best vein to vein time. As a company matures, it’s important to proactively and routinely review the supply chain design and key business practices to ensure they still support customer needs effectively and efficiently.
AIM publishes information and resources related to supply chains for a wide range of biopharma products, including cell and gene therapies. Please follow our LinkedIn page or visit our Insights page to stay up to date. To discuss the contents of this article, or to inquire about how AIM can help you design and develop the optimum supply chain for a cell-based therapy, please contact us here.
To receive a copy of this article in PDF format, download the white paper here.
[1] Note that if a company holds its own MIA, then in most cases it will not need a separate WDA for that specific entity.